Although a significant number of jurisdictions exist globally in which voluntary assisted dying has been legalised, there is little research and no guidance on how to care for patients’ spiritual needs in the voluntary assisted dying environment. Voluntary assisted dying (VAD) refers to the lawful process by which a person with a life-limiting illness may choose to end their life, under strict eligibility and procedural requirements. In Australia particularly, VAD is legislated on a state-by-state basis, resulting in variable eligibility criteria, clinical responsibilities, and safeguards, which can significantly affect the experiences of patients and families. Evidence indicates that spiritual wellbeing is a crucial element of holistic health (Koenig, 2012; Page et al., 2020), and the World Health Organization has acknowledged this (World Health Organization, 2021, p. 2). Many health care practitioners also view spiritual care as a foundational ethical obligation (Pesut, 2006; Soheili & Mollai Iveli, 2019).
Systematic reviews have identified that spiritual care provision is associated with patients’ choice to access VAD (Gerson et al., 2020); moreover, it is significantly beneficial to VAD patients and their families, regardless of their identification with religion or lack thereof (Oczkowski et al., 2021). This evidence indicates spiritual care plays a critical role in the overall wellbeing of VAD patients and their families but current research, to the knowledge of the authors, has not comprehensively identified what existential or spiritual challenges a patient may face in the VAD environment or what mechanisms a spiritual care practitioner could use to assist a patient. However, current research does offer indicators that spiritual care in the VAD environment is important and requires a holistic approach (see Li et al., 2014, for example), emphasising both internal and relational spiritual concerns.
Unique Spiritual Care Challenges Associated With Voluntary Assisted Dying
When addressing existential concerns, defining the existential or spiritual is paramount. Therefore, this article will not focus on the folk idea of religion or the concept of religiosity, but rather phenomena associated with spirituality and existential experiences (Paloutzian & Park, 2021). This can include experiences such as feelings of love beyond the self and for all humanity, deep and intimate connections with others in a given moment, and a sense of correspondence or attachment to the divine or transcendent. Multiple frameworks have been proposed to account for these experiences, such as the qualitative work of Koper et al. (2019) and the quantitative work of Rovers and Kocum (2010) or Kielkiewicz et al. (2019). In these frameworks, a consistent theme arises of spirituality as an internal existential construct that is socially situated and influenced. The social nature of spirituality is generally common to all relevant conceptual frameworks; however, Kielkiewicz et al. (2019) uniquely conceptualised spirituality as purely internal, influenced only by relational and communal factors, not derived from them. Drawing on this previous work, strategies to provide counsel to patients on existential challenges associated with VAD should define spiritual concerns not only as internally derived phenomena but also as rooted in community and relational dynamics.
It is worth acknowledging that much of the evidence used to support VAD spiritual care practices in this article is drawn from the palliative care environment; nonetheless, the VAD and palliative care environments differ significantly. No research has definitively identified the transferability of spiritual care practices between the palliative care and VAD environments (Gerson et al., 2020). While this does not reject transferability, assumptions of transferability lack acknowledgement of the differing motivations and goals of care between palliative care and VAD environments. These hidden factors may produce effects detrimental to patient care. Exemplifying the differing motivations between palliative care and VAD is the observation that Australian palliative care specialists are significantly more likely to refuse involvement in the VAD treatment process than are other practitioners (Rutherford et al., 2021; Sellars et al., 2021); this also holds true for geriatricians and oncologists (Rutherford et al., 2021). Not all health practitioners hold the same philosophical positions, and not all health environments have the same clinical goals. Despite the use of similar therapeutic approaches in both VAD and palliative care environments, different causes for patient distress are often present between these environments, and effective treatment incorporates the differences between VAD and palliative care to improve patient wellbeing effectively (Saracino et al., 2019). Extending from this principle, palliative care and VAD almost certainly elicit different existential and spiritual questions in patients, their family, and their community. Whereas a degree of similarity between palliative care and VAD environments is highly likely, acknowledgement of difference is imperative, and the lack of empirically identified differences can produce issues in treatment planning.
VAD is a distinctly controversial practice between health practitioners and in the wider community, and spiritual care practitioners need to be aware of this to deliver effective care. VAD presents unique moral, ethical, and emotional issues that health practitioners reckon with on an individual level (Evenblij et al., 2019; Kelly et al., 2020; Pesut et al., 2020; Sellars et al., 2021). VAD is also not unanimously accepted by every culture, religious tradition or philosophical worldview (Liégeois, 2022; Mehra & Avasthi, 2021; Nissanka, 2022; Vlad (Chirvăsuță), 2022); hence, the VAD environment must be treated as extremely sensitive; that is, it has a significant capacity to contribute to spiritual, existential, and emotional harm for patients, families, communities, and health practitioners. Moreover, different sociocultural systems regard the idea of a dignified death differently (Li et al., 2014), and effective spiritual care should account for this. All VAD spiritual care should consider the current and historical controversy of VAD itself to meet the unique sociocultural, emotional, and spiritual needs of patients.
Addressing the Internal Spiritual Concerns of Patients
When addressing internal spiritual concerns of patients accessing VAD, it is critical that a sense of internal congruence, particularly concerning VAD choices, be established. Schuhmann et al. (2021) released a rare VAD spiritual care case study, and their patient derived significant therapeutic benefit from the spiritual care practitioner facilitating a narrative exploration of the patient’s life and how VAD was situated in that story. This assisted the patient to reconcile VAD with their broader life history and existential belief system to establish a sense of internal congruence. The process facilitated a sense within the patient that VAD was consistent with their existential beliefs and did not contradict other elements of their sense of self-improved wellbeing. Generalising from this case study alone is highly speculative, yet the case study echoes themes from the broader literature. Individuals whose belief systems are congruent with their actions and sense of self manage existential fears better, including fears of death (Ardelt & Koenig, 2006; Kukulka et al., 2019; Page et al., 2020); they also tend to experience improved psychological wellbeing more broadly (Ardelt & Koenig, 2006; Daigle, 2019). Spiritual beliefs can cause distress instead of comfort when there is a contrasting sense of incongruence or conflict within a person. Such senses of incongruence can include experiencing a feeling of divine abandonment while also believing in an unconditionally loving God or feeling an impression of damnation emanating from incongruence between moral beliefs and actions (Page et al., 2020). While all the mechanisms affecting spiritual wellbeing in the VAD environment are yet unknown, a sense of internal congruence between existential beliefs and personal action appears to have a significant positive impact on how patients spiritually reckon with their VAD decision-making.
Making meaning out of the VAD end-of-life experience is also essential for patients’ spiritual health. Rovers and Kocum (2010) identified meaning-making as an important element of how spirituality creates hope, and this principle has held true in end-of-life environments (Ardelt & Koenig, 2006; Olsman et al., 2014; Wakefield et al., 2018). However, owing to the curative implications of the term “hope” in a health care environment (Lohne, 2022), a focus on existential and spiritual meaning may be more applicable to meaning-making and hope in the VAD environment. Olsman et al. (2014) related meaning-making to an individual’s personal narrative, and it would be poorly conceived to argue that existential meaning-making is not intertwined with personal narrative congruence. The VAD experience itself has a significant place in a patient’s personal narrative, but potentially also independently comprises a meaningful existential experience that can promote or undermine spiritual wellbeing. This meaning-making aspect of the VAD experience cannot be prescribed and requires individualised care that is attentive to the patient’s sociocultural and existential context (Li et al., 2014). Although mechanisms of meaning-making have not been explicitly studied in the VAD setting, there is evidence that meaning-making is important for the patient’s experience in many end-of-life environments; therefore, spiritual care practitioners need to address what the VAD experience independently means to a patient, as an extension of how it fits into their personal narrative.
Addressing the Relational Spiritual Concerns of Patients
When familial congruence and effective communication are present, family members serve a vital psychosocial support function within end-of-life care settings (McCauley et al., 2021). Disruptions in family congruence and communication often significantly diminish the psychologically fortifying effect familial relationships provide to a patient (Kukihara et al., 2020). Familial incongruence could potentially be derived from disagreement about accessing VAD or miscommunicating emotional needs. To optimise patient wellbeing throughout the VAD end-of-life experience, spiritual care practitioners should tend to and cultivate patients’ familial relationships. Caring for and fostering family relationships in difficult settings is not unprecedented in spiritual care (Willemse et al., 2020). Psychoeducational techniques can be used by professionals to increase patient–family congruence in end-of-life care decisions (Jung & Matthews, 2021). Increasing patient–family communication quantity and quality generally increases patient wellbeing in end-of-life care (Jung & Matthews, 2021). Family support is essential to patient wellbeing throughout the end-of-life experience, and this support can be disrupted because of decisional incongruence or general miscommunication; spiritual care practitioners need to support these relationships as a foundational element of patient care.
Reduction in the wellbeing of family members can diminish their capacity to provide psychosocial support to a patient; therefore, spiritual care practitioners should consider the wellbeing of family members when supporting a patient’s end-of-life experience. A systematic mixed-studies review in the Netherlands, where VAD has been legal since 2002, identified that while the VAD environment often involves supporting a patient–family–physician triad, the Dutch legal framework only recognises a patient–physician dyad (Roest et al., 2019). The VAD environment most often does not accommodate family-based shared decision-making, only recognising decision-making authority within a patient–physician dyad; this produces a uniquely distressing power imbalance for family members that disagree with the patient’s choice to access VAD (Variath et al., 2020). This contrasts with most end-of-life care environments in Australia, wherein families develop decision-making partnerships with clinicians, which tends to improve family wellbeing (Gonella et al., 2019). If a family member is experiencing poor wellbeing concerning their decision-making power owing to the exclusionary nature of the VAD environment, that will have negative effects on patient wellbeing through the mediating influence of family dynamics because the family member will experience a diminished capacity to provide psychosocial support (Kukihara et al., 2020). Patient medical autonomy cannot usually be undermined for the sake of a family member’s wellbeing since accessing VAD is generally a patient’s legal right. However, it is imperative that the effect of poor family wellbeing on patients be addressed. Caring for family members’ wellbeing and existential concerns, if not a legitimate practice in and of itself, is vital for supporting the wellbeing of a patient through the mediating influence of family dynamics. Such family-focused care will likely be needed often owing to the uniquely challenging nature of elements of the VAD environment.
Given the potential for tension between a patient’s end-of-life decisions and the doctrinal positions of their spiritual or religious community, it is critical that spiritual care practitioners navigate these relationships with both sensitivity and discernment. Directly confronting or challenging a spiritual leader’s beliefs to advocate for a patient’s choice regarding VAD may inadvertently compromise the patient’s access to spiritual or communal support. In this context, spiritual care practitioners are encouraged to act as mediators—supporting patient autonomy alongside fostering respectful dialogue with religious leaders to preserve vital relational and existential resources for the patient. This concern is underscored by institutional guidance such as that from Catholic Health Australia (2021), which explicitly opposes VAD but nonetheless urges its pastoral workers to accompany patients with compassion and without judgement. Similarly, Lutheran aged care institutions in South Australia have acknowledged the challenge of developing VAD policies that respect both denominational ethics and the legal rights of residents, highlighting the importance of nuanced, values-based care (Lutze, 2023). Such evidence suggests that when theological objections exist, spiritual care practitioners are more likely to sustain meaningful spiritual support for patients by prioritising dialogue and mutual respect over confrontation. This aligns with broader ethical frameworks in spiritual care, which advocate for non-coercive, patient-centred engagement grounded in professional integrity and relational trust.
Holistic Spiritual Care in the Voluntary Assisted Dying Environment
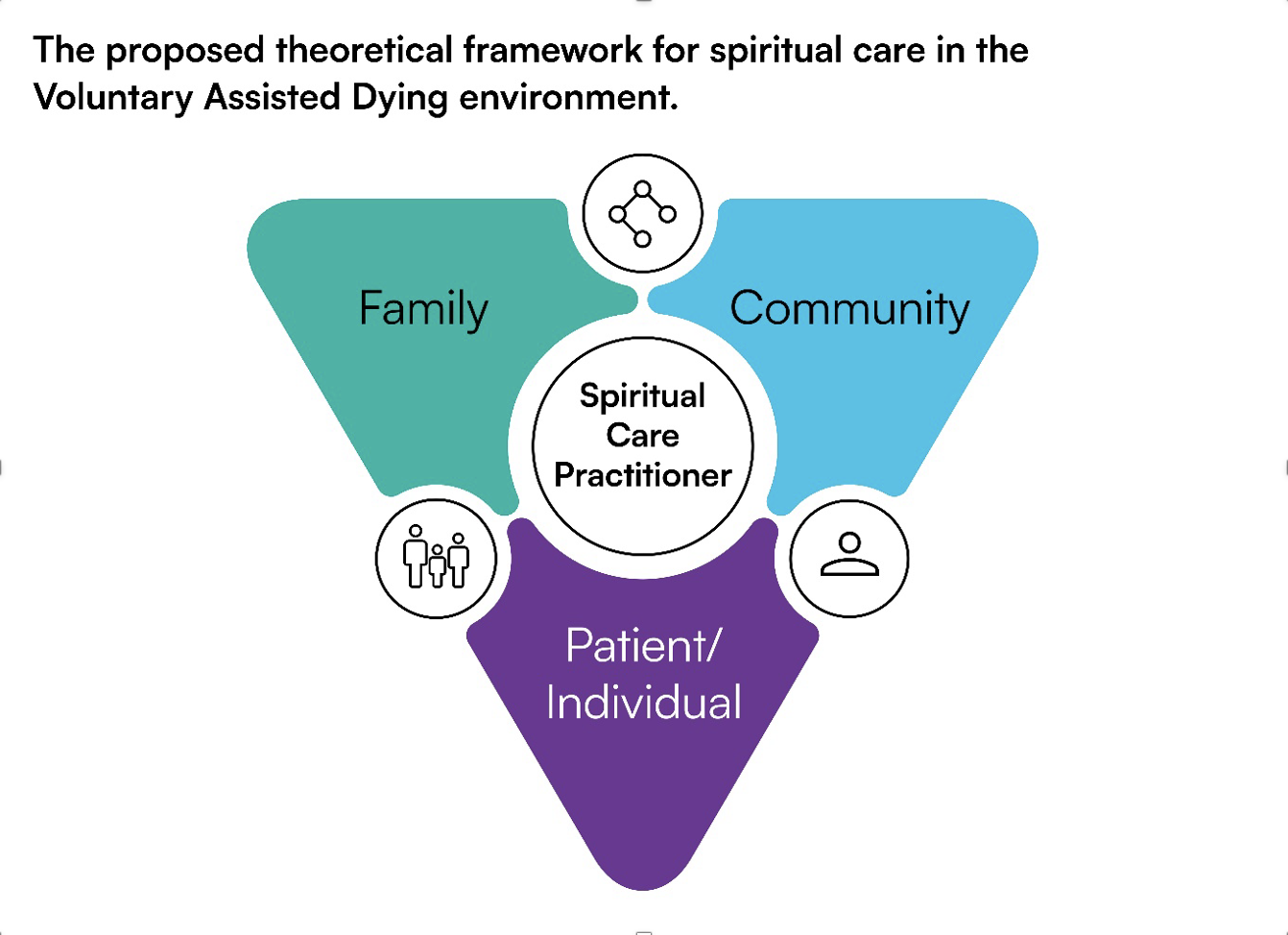
Owing to the impact on the quality of a patient’s end-of-life experience that family, community, and other significant patient relationships can have, spiritual care practitioners must conceptualise a patient’s spiritual concerns through both relational and internal lenses. Spiritual care practitioners are generally expected to act in a way that does not compromise or disrespect the beliefs of anyone (Spiritual Care Australia, 2023, pp. 6–7), while still attending to each person’s individual needs (see Figure 1).

Therefore, a spiritual care practitioner can exist in the nexus of a patient’s interacting relationships, acting to support the relationships and optimise their beneficial impact on a patient’s wellbeing. For example, this may include psychoeducation to increase familial congruence and addressing personal patient concerns to maximise the benefits of both interventions. It appears best to address a patient’s internal spiritual concerns in tandem with their relational concerns and any corresponding relational spiritual questions. Evidence to support spirituality’s relational nature is plentiful (Batstone et al., 2020; Bush & Bruni, 2008) and spiritual care practitioners should almost certainly view themselves as holistically supporting a patient’s relationships alongside their internal existential needs to achieve the greatest therapeutic effect.
Conclusion
Although research on spiritual care in the VAD environment is scant proportional to available samples, the existing literature suggests that therapeutically intervening to support both internal spiritual concerns and a patient’s relationships is necessary to optimise wellbeing. When addressing a patient’s internal existential concerns, establishing a sense of congruence between the process of accessing VAD and a patient’s broader personal narrative is crucial. Intertwined with a patient’s personal, independent narrative is ongoing encouragement from a spiritual care practitioner for the patient to make meaning of the VAD experience itself. A practitioner should address the relationship between a patient and their family, attempting to establish communicative and supportive relationships within family dynamics. Ultimately, such interventions aim to increase not only familial congruence but also, through the mediating influence of family dynamics, the psychosocial support family provides to a patient. Throughout all of this, it is vital that a spiritual care practitioner is mindful of the uniquely controversial and distressing nature of the VAD environment for many people and communities. Care plans may necessitate acknowledgement of religious, spiritual or philosophical sensitivities concerning VAD. Finally, supporting the relationship between an individual and their personal community spiritual carer is essential, if applicable, because spiritual communities can provide vital end-of-life support (Balboni et al., 2007, 2022). This places the spiritual care practitioner in a nexus of interacting patient relationships in the VAD environment. Future research is recommended to identify effective interventions for holistic internal and relational spiritual care that do not compromise a patient’s significant relationships or existential concerns but work with the unique concerns associated with the VAD environment.